Knee Replacement Surgery: A Complete 2026 Patient Guide
Knee pain can gradually take over your daily life. Even a short walk can leave you tired. You might start avoiding stairs, have trouble sleeping, and need to plan just to get out of a chair.
If medication, exercise, injections, and other treatments stop working well enough, knee replacement surgerymight be considered. While it is a major surgery, most people find real pain relief and better movement afterward.
Recovery requires effort and patience. The new knee will not feel just like a natural, healthy joint, and results are different for everyone. Knowing this can help you prepare and set realistic goals.
Medical note:This article provides general information. Your orthopedic surgeon and healthcare team should guide decisions about treatment, medications, surgery, and rehabilitation.
What Is Knee Replacement Surgery?
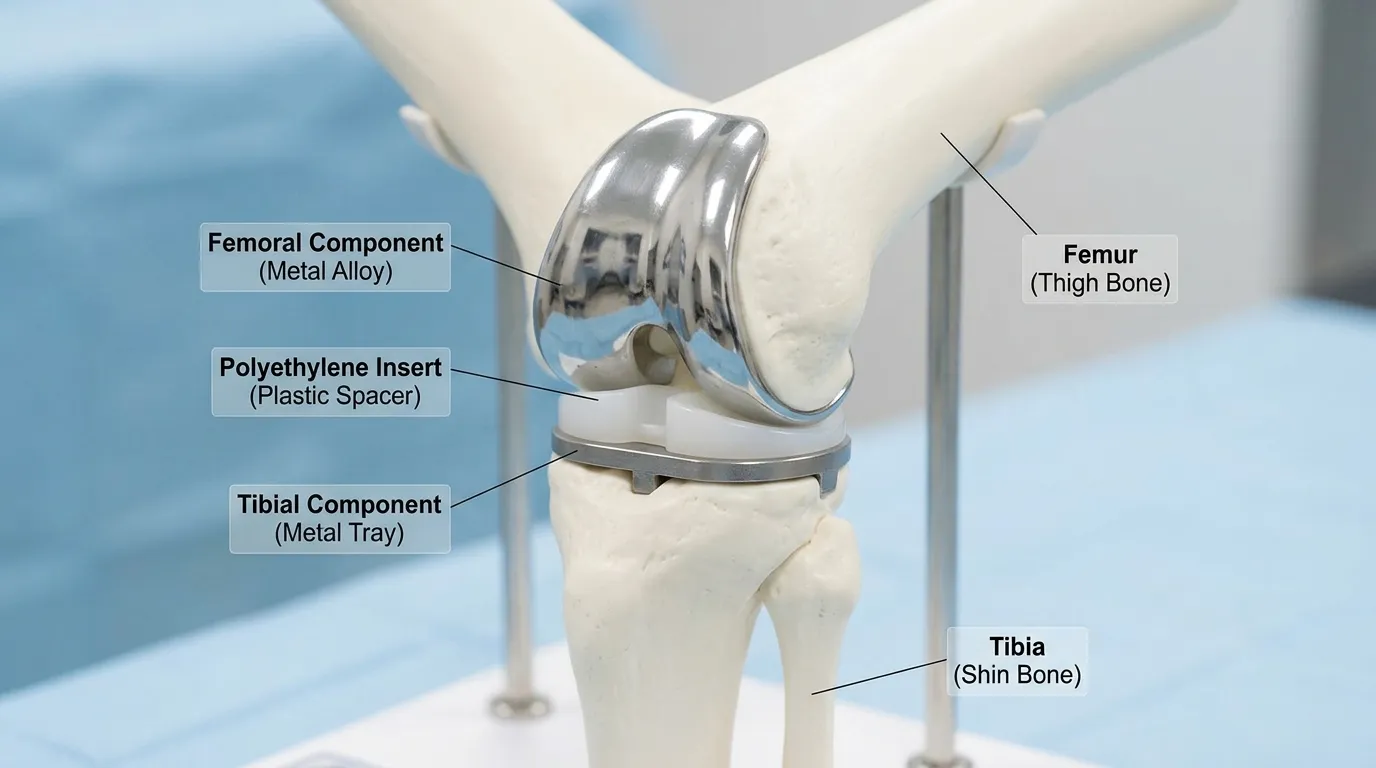
Knee replacement surgery is an operation that removes damaged cartilage and a small amount of bone from the knee, then covers those surfaces with metal and medical-grade plastic components.
The medical name for this surgery is knee arthroplasty. Despite the name, the surgeon does not remove your whole knee. Instead, the procedure is more like resurfacing the damaged ends of your thighbone and shinbone.
A plastic spacer sits between the metal components so the joint can move smoothly. The underside of the kneecap may also be resurfaced, depending on the patient and the surgeon’s technique.
Most surgeries last about one to two hours. Some people go home the same day, while others stay in the hospital overnight or longer, depending on their health, mobility, pain control, and support at home.
Why Is Knee Replacement Surgery Performed?
The main goals are to reduce long-term pain, improve movement, correct serious deformity, and make daily activities easier.
Osteoarthritis
Osteoarthritis is the most common reason for knee replacement. The protective cartilage covering the joint gradually wears down. As the damage becomes severe, the bones may rub against each other.
This can cause pain, stiffness, swelling, reduced movement, and a bowed or knock-kneed appearance.
Inflammatory arthritis
Conditions such as rheumatoid arthritis can inflame the joint lining and damage cartilage and bone. Surgery may be considered when joint destruction causes persistent pain and disability.
Patients taking immunosuppressive medication need an individual plan for managing these medications around surgery.
Post-traumatic arthritis
A previous fracture, ligament injury, meniscus injury, or other serious knee trauma may change the way force passes through the joint. Arthritis can develop years later.
Other causes
Less common reasons include osteonecrosis, severe knee deformity, certain childhood joint disorders, and failure of a previous knee replacement.
Who May Be a Candidate for Knee Replacement Surgery?
There is no single test that determines whether someone needs a knee replacement. The decision usually combines symptoms, examination findings, X-rays, previous treatment, general health, and personal goals.
Common signs that surgery may be appropriate include:
Severe pain that limits walking, stairs, work, sleep, or basic household tasks.
Pain while resting, including at night
Ongoing stiffness or swelling
Difficulty getting out of chairs or entering a car
A knee that bows inward or outward
Instability or a feeling that the knee may give way
Moderate-to-severe damage visible on X-rays
Inadequate relief from suitable nonsurgical treatments
Doctors usually recommend surgery based on pain and how much it limits your life, not just your age. There are no strict age or weight limits for everyone, but both can affect surgery risks and how long the implant lasts.
Treatments usually tried before surgery.
Depending on the condition, earlier treatment may include:
Activity changes
Weight management
Strengthening and low-impact exercise
Physical therapy
Walking aids or a brace
Acetaminophen or anti-inflammatory medication when medically appropriate
Corticosteroid or other joint injections
Patients with advanced arthritis do not always benefit from repeating treatments that have already failed. Current ACR and AAHKS guidance conditionally recommends that patients with moderate-to-severe symptoms, consistent X-ray findings, and an unsuccessful trial of appropriate nonsurgical care should not automatically be forced to delay surgery for additional physical therapy, anti-inflammatory drugs, braces, or injections. The final decision still requires shared decision-making.
Health issues that may need attention first
An orthopedic team may recommend improving certain health risks before surgery, including:
Poorly controlled diabetes
Nicotine use
Active infection
Untreated skin wounds near the knee
Significant anemia
Serious heart, lung, kidney, or circulation problems
Poor nutrition
Unmanaged dental infection
Having a higher body weight can raise the risk of infection and other problems. Still, strict BMI limits do not fit everyone, and waiting to reach a certain number does not always lead to better results. It is often more important to focus on controlling diabetes and stopping nicotine use before surgery.
Types of Knee Replacement Surgery
The amount and location of joint damage help determine which operation is suitable.
Total knee replacement | The damaged surfaces across the main knee compartments | Patients with widespread arthritis or deformity | Most common option; longer recovery than a limited replacement |
Partial knee replacement | One damaged compartment, usually the inner side | Patients with arthritis limited to one area and suitable ligaments | Smaller operation and often faster early recovery, but arthritis can later develop elsewhere |
Patellofemoral replacement | The joint between the kneecap and thighbone | Selected patients with isolated kneecap-joint arthritis | Preserves healthy parts of the knee; not suitable when damage is widespread |
Revision knee replacement | Some or all parts of an earlier implant | Patients with infection, loosening, instability, wear, fracture, or persistent implant problems | Usually more complex than the first operation and may require larger implants or bone grafting |
Total knee replacement
Total knee replacement is used when arthritis affects several parts of the joint. The surgeon resurfaces the lower end of the femur and upper end of the tibia, inserts a plastic bearing, and decides whether the kneecap should also be resurfaced.
Partial knee replacement
A partial or unicompartmental replacement preserves more natural bone and ligaments. Patients often have less early pain and swelling than those undergoing total replacement.
It is only suitable when damage is confined to a limited area, and the remaining joint structures are healthy enough to support it.
Patellofemoral replacement
This operation treats arthritis limited to the space behind the kneecap. It is less common because many patients also have damage elsewhere in the knee.
Revision knee replacement
Revision surgery removes or changes an existing implant. It may be needed due to infection, loosening, instability, fracture, wear, stiffness, or ongoing pain related to an implant problem.
Revision procedures often take longer and carry greater risks than a first knee replacement.
Is robotic knee replacement a different type?
Robotic or computer-assisted surgery is a method of planning and positioning the implant, not a separate type of replacement.
These systems can improve measurement and alignment accuracy. However, current evidence has not consistently shown better short- or medium-term function, implant survival, or complication rates compared with well-performed conventional surgery. Surgeon experience, patient selection, implant choice, and rehabilitation remain important.
How to Prepare for Knee Replacement Surgery
Preparing well can help make your first weeks at home safer and less stressful.
Complete the medical evaluation.
Your preoperative assessment may include:
A medical history and physical examination
Blood tests
An electrocardiogram
Knee X-rays
Additional imaging for selected procedures
A review of heart, lung, kidney, or other chronic conditions
Infection screening when required
Let your healthcare team know about all the prescription and over-the-counter medicines, vitamins, and supplements you use. Some of these can increase bleeding, affect anesthesia, or interact with medicines you will need after surgery.
Do not stop blood thinners, diabetes medication, steroids, or other important medicines without specific instructions.
Discuss dental and skin problems.
Tell the surgical team about tooth infections, major planned dental work, rashes, cuts, insect bites, sores, or other skin damage. An active infection or break in the skin can lead to postponement because bacteria may reach the new joint.
Reduce nicotine use
Smoking and other nicotine products can interfere with blood flow, wound healing, and infection prevention. Your team may recommend reducing or stopping nicotine before the operation and during recovery.
Manage diabetes
Blood sugar control matters before and after surgery. Poor control is linked to worse healing and a higher risk of infection.
There is no single blood sugar or HbA1c cutoff that fits every patient. The surgeon, primary care clinician, and diabetes specialist should agree on a safe plan.
Work on strength and mobility
A pre-surgery exercise program may focus on the quadriceps, hips, core, upper body, balance, and walking tolerance.
Pre-surgery exercises cannot reverse advanced arthritis, but getting stronger can make it easier to move, use a walker, and start rehab. Exercises should be chosen based on your pain and physical condition.
Prepare the home
Useful changes include:
Remove loose rugs, cords, and clutter.
Make clear paths for a walker.
Add secure stair railings.
Place frequently used items within easy reach.
Arrange a firm chair with arms.
Consider a shower chair, raised toilet seat, or grab bars.
Set up a sleeping space on the main floor when stairs are difficult to navigate.
Arrange transportation and help with meals, pets, errands, and medications.
Most people need help for at least the first few days after surgery. Some will need support for a few weeks.
Plan for the first week.
Before surgery, make sure you understand:
Which medicines to take or stop
When to stop eating and drinking
Which pain medicines may be prescribed?
How blood clots will be prevented
When physical therapy begins
How the dressing should be managed
Who to call after hours
Whether the operation is planned as same-day or inpatient surgery
What Happens During Knee Replacement Surgery?
The exact process varies, but most operations follow the same general stages.
1. Anesthesia is given
Patients usually receive either general anesthesia or regional anesthesia.
General anesthesia keeps the patient unconscious. Regional anesthesia, often a spinal anesthetic, numbs the lower half of the body. Sedation may also be given.
A nerve block or local anesthetic around the knee can help control pain after surgery. The safest plan depends on medical history, medication use, previous spine surgery, and personal preferences.
2. The surgeon reaches the joint
An incision is made at the front of the knee. The surgeon moves the kneecap aside to reach the damaged surfaces.
3. Damaged bone and cartilage are removed
Thin sections of worn cartilage and underlying bone are cut from the femur and tibia. The surgeon also removes bone spurs and balances the soft tissues.
4. Trial components are tested
Temporary components help the surgeon check implant size, stability, alignment, bending, straightening, and ligament balance.
5. The permanent components are secured
Metal components are attached to the femur and tibia. They may be fixed with bone cement or placed with a porous surface that allows bone to grow into the implant.
A strong plastic spacer is inserted between them.
6. The kneecap is assessed
The underside of the kneecap may be resurfaced with a plastic component. Patellar resurfacing is not required in every operation.
7. The incision is closed
The surgeon closes the deeper tissues and skin, then applies a sterile dressing.
Antibiotics, early movement, mechanical compression, and blood-thinning medication may be used to lower infection and clot risks.
Knee Replacement Surgery Recovery Timeline
Recovery does not always move forward in a straight line. You might have a good day, then feel more swelling or tiredness after doing more activity.
The following timeline is a guide, not a deadline.
Day 0 to 2 | Standing and walking with help; pain, swelling, and fatigue; beginning simple exercises; same-day or hospital discharge when safe |
Week 1 to 2 | Frequent short walks; walker use; wound care; scheduled exercises; regular icing and elevation; help may still be needed |
Week 3 to 6 | Gradual transition to a cane or no walking aid; better household mobility; possible return to desk work; driving may be considered after medical clearance |
Week 7 to 12 | Improved strength and range of motion; longer walks; easier daily activities; continued physical therapy where needed |
Month 3 to 6 | Major gains in endurance and confidence; return to more low-impact recreation; occasional stiffness or swelling may continue |
Month 6 to 12 | Ongoing improvement in strength, comfort, balance, and function; many patients approach their final result |
Many people get back to most of their normal routine in about six weeks, but full recovery can take six to twelve months. How long it takes depends on your fitness before surgery, age, other health issues, any complications, your job, and the type of knee replacement you have.
When can patients walk?
Walking usually begins on the day of surgery or the following day, using a walker or crutches.
Some patients move to a cane within two to three weeks. Others need an assistive device longer. The important goal is a safe, balanced walking pattern, not abandoning the walker as quickly as possible.
When can patients drive?
Many patients return to driving around four to six weeks after surgery, but timing varies.
Patients should not drive until they:
Are no longer taking medicines that impair alertness
Can enter and exit the car safely
Can control the pedals
Have regained enough strength and reaction time
Have been cleared by their surgeon
Recovery may be faster if the surgery was on your left knee and you drive an automatic car. Be sure to check your insurance rules as well.
When can patients return to work?
A desk-based job may be possible after roughly four to six weeks. Work involving prolonged standing, lifting, climbing, kneeling, or travel may require up to three months or longer.
Rehabilitation After Knee Replacement Surgery
Rehabilitation begins soon after surgery because moving helps your blood flow, reduces stiffness, and rebuilds muscle strength.
The program should be individualized. A patient recovering from a partial replacement may progress differently from someone who had a complex total or revision procedure.
Main rehabilitation goals
Physical therapy commonly works toward:
Fully straightening the knee.
Gradually increasing bending
Activating the quadriceps
Improving hip and leg strength
Walking without a limp
Managing stairs safely
Restoring balance
Returning to daily tasks and suitable exercise
Exercises may include ankle pumps, quadriceps contractions, heel slides, supported knee bends, straight-leg raises, sit-to-stand practice, and progressive walking. Only perform exercises approved by the surgical or therapy team.
How much pain is normal during therapy?
Stretching and strengthening can cause soreness. Sharp pain, sudden loss of function, unusual instability, or swelling that keeps increasing should not be treated as something to push through.
A common mistake is avoiding movement because it hurts. Doing too much is also a problem, as it can cause more swelling and make your next therapy session harder.
A steady program usually works better than occasional intense exercise.
What if the knee stays stiff?
Some stiffness is expected early. The surgeon should be informed if bending or straightening no longer improves despite consistent rehabilitation.
For selected patients with significant scar-related stiffness, manipulation under anesthesia may be considered. When needed, outcomes are generally better when performed within about 3 months of the replacement.
Expected Results After Knee Replacement Surgery
The main benefit is pain relief. Most patients also walk more comfortably, perform daily tasks more easily, and report better quality of life.
A successful replacement may allow a patient to return to:
Regular walking
Swimming
Cycling
Golf
Light hiking
Dancing
Gardening
Other low-impact exercise
Research shows that about 10% of people are not satisfied after knee replacement, meaning most are happy with the results, but some are not. Ongoing pain, stiffness, unrealistic expectations, other health problems, and complications can affect how you feel about the outcome.
What the operation may not change
A replacement is unlikely to feel exactly like the knee did before arthritis.
Some patients continue to notice:
Numbness near the scar
Clicking or other mechanical sensations
Mild swelling after activity
Difficulty kneeling
Reduced deep bending
Occasional stiffness
Some remaining pain
Most surgeons advise avoiding regular running, jumping, and other high-impact sports because repeated heavy impact may increase wear or loosening. Walking, swimming, cycling, golf, and similar lower-impact activities are usually more suitable.
Risks and Potential Complications
Knee replacement is usually safe, but every major surgery has some risks. Your personal risk depends on things like your age, health conditions, nicotine use, blood sugar control, weight, any previous surgeries, and how complex your procedure is.
Infection
Infection can affect the skin or develop deep around the implant. Deep infection may require prolonged antibiotic therapy, joint-cleaning surgery, or removal and replacement of the components.
The average infection risk is commonly estimated at around 1% to 2%.
Blood clots
A clot can form in a deep vein of the leg. If it travels to the lungs, it can cause a pulmonary embolism.
Risk reduction may include:
Early walking
Ankle movement
Compression devices or stockings
Blood-thinning medication
Adequate hydration
Avoiding prolonged immobility
The exact prevention plan should be based on both clotting and bleeding risk.
Bleeding and anemia
Some blood loss is expected. Significant bleeding or the need for transfusion is less common than it was with older techniques, but it remains possible.
Stiffness
Scar tissue can limit bending or straightening. Early movement and rehabilitation reduce the risk, although stiffness can still occur despite good participation.
Persistent pain
Some patients continue to experience pain after apparently successful surgery. Possible causes include stiffness, instability, infection, implant problems, nerve pain, hip or spine conditions, or pain that cannot be traced to a single structural problem.
Nerve or blood vessel injury
Nerves and blood vessels around the knee can be stretched or injured. Serious injury is uncommon, but temporary numbness around the incision is frequent.
Implant problems
Components may loosen, wear, shift, or become unstable. A fracture can also occur around the implant, particularly after a fall or in weaker bone.
Medical complications
Possible complications include:
Reaction to anesthesia
Heart attack
Stroke
Kidney problems
Lung complications
Urinary problems
Medication side effects
Serious medical complications are uncommon but may be more likely in patients with complex health conditions.
Long-Term Outcomes
Modern knee replacements often last 20 years or more. One large study found that about 82% of knee replacements were still working after 25 years. These numbers are averages, so your own results may vary.
Longevity can be influenced by:
Age at the time of surgery
Activity level
Body weight
Implant design and fixation
Surgical positioning
Bone quality
Infection
Falls or fractures
Regular high-impact activity
Younger patients have more years in which the implant can wear or loosen, so their lifetime chance of revision may be higher.
Caring for the replacement
Long-term care usually includes:
Maintaining a healthy body weight
Staying active with lower-impact exercise
Building leg strength and balance
Reducing fall risk
Treating skin, urinary, and dental infections promptly
Telling healthcare professionals about the implant
Attending follow-up visits recommended by the surgeon
Antibiotics before dental work are not automatically needed for every joint replacement patient. Ask the orthopedic surgeon and dentist whether personal health risks make them appropriate.
When to Contact a Healthcare Provider
It is normal to have some pain, warmth, bruising, and swelling in the early days after surgery. These symptoms should slowly get better over time.
Contact the surgical team promptly for:
Redness, warmth, swelling, or pain that is worsening
Pus, unpleasant odor, or increasing wound drainage
Persistent fever or shaking chills
Bleeding that soaks through the dressing.
Pain not controlled by the prescribed plan.
New calf pain, tenderness, redness, or swelling
A foot that becomes unusually cool, dark, pale, or numb
Sudden loss of movement or stability
A fall onto the operated leg
An unexpected decline after the knee had been improving.
Seek emergency care for:
Sudden shortness of breath
Chest pain
Chest pain made worse by coughing or breathing
Coughing up blood
Fainting or collapse
These can be signs of a clot that has reached the lungs and require immediate assessment.
Common Recovery Mistakes
Comparing progress with another patient
Two people can have the same procedure and recover at different speeds. Preoperative strength, swelling, pain sensitivity, sleep, medical conditions, and surgical complexity all matter.
Stopping the walking aid too early
Using a cane or walker is not a failure. A safe walking pattern protects the knee and reduces the risk of falls.
Doing too much on a good day
If you suddenly do a lot more walking, errands, or exercise, you might end up with more pain and swelling. Try to increase your activity slowly and steadily.
Skipping pain medication until pain is severe
Take pain medicine only as your doctor prescribes, but do not wait until the pain is severe before taking it. This can make it harder to move and sleep. Ask your care team about a safe schedule and how to reduce your medication when the time comes.
Ignoring constipation
Opioid medication, reduced movement, and dietary changes commonly cause constipation. Discuss fluids, food, movement, and a preventive bowel plan before leaving the hospital.
Expecting the knee to feel normal in a few weeks
You will likely get back to most daily activities before your knee is fully healed. Swelling, tiredness, trouble sleeping, and stiffness can last for several months.
Pushing through warning signs
Rehabilitation discomfort and complication symptoms are distinct. Worsening drainage, fever, calf pain, chest pain, or sudden shortness of breath need medical attention.
Frequently Asked Questions
How painful is knee replacement surgery?
Moderate-to-severe pain is expected during the first part of recovery, especially in the first few days and during early movement. A combination of anesthesia, nerve blocks, acetaminophen, anti-inflammatory medicine when safe, and short-term opioid medication may be used.
Pain should gradually become more manageable. Severe pain that does not respond to the prescribed plan needs medical review.
How long does it take to walk normally after knee replacement surgery?
Walking with assistance often begins within 24 hours. Many patients progress from a walker to a cane over the following weeks.
Walking without a limp may take several weeks or months. Strength, balance, swelling, and preoperative walking habits affect the timeline.
What is the hardest part of knee replacement recovery?
The first few weeks are often the hardest because pain, swelling, fatigue, poor sleep, medication side effects, and daily exercise all occur at the same time.
Having realistic expectations, support at home, a clear plan for your medicines, and staying in touch with your care team can help make this stage easier.
How long does knee replacement surgery take?
The operation itself typically takes about 1 to 2 hours. Preparation, anesthesia, and recovery-room monitoring add several more hours to the hospital visit.
Is total or partial knee replacement better?
Neither is automatically better.
Partial replacement can preserve more natural tissue and may offer faster early recovery, but it only works for carefully selected patients with damage limited to one part of the knee. Total replacement is usually more appropriate when arthritis affects several compartments.
What age is best for knee replacement surgery?
There is no universal best age. The decision should be based on the severity of symptoms, joint damage, health risks, previous treatment, daily limitations, and personal goals.
A younger person may recover well but has a greater lifetime chance of needing revision surgery.
Can both knees be replaced at the same time?
Simultaneous bilateral replacement is possible, but it places greater demands on the heart, lungs, blood supply, rehabilitation, and home support.
Many patients have the operations separately. The safest approach depends on health, age, surgical risk, and the severity of both knees.
Is robotic knee replacement better?
Robotic assistance can help with surgical planning and precise component positioning. It has not consistently produced better long-term function or implant survival than conventional surgery.
Ask how frequently the surgeon uses the system, why it is recommended for your knee, whether extra imaging is needed, and whether it changes the cost.
Can you kneel after a knee replacement?
Many patients can kneel safely after healing, but kneeling may feel uncomfortable or unnatural due to scar sensitivity, numbness, pressure, or limited range of motion.
A therapist can provide a gradual, protected way to practice once the surgeon confirms that the wound and tissues have healed.
How long will a knee replacement last?
Many implants last 20 years or longer. Activity, age, weight, implant fixation, infection, injuries, and other factors affect longevity.
Can knee replacement surgery fail?
Yes, although most replacements function well for many years. Failure can result from infection, loosening, wear, instability, fracture, stiffness, or persistent pain. Some problems require revision surgery.
Final Thoughts on Knee Replacement Surgery
Knee replacement surgerycan give lasting pain relief and better movement when severe joint damage makes daily life hard and other treatments are no longer enough.
This surgery is not a quick fix. It takes careful planning, early movement, months of steady rehab, and realistic expectations. Most people get better, but the knee may still have some stiffness, numbness, swelling, or a sense of the implant.
The best choice is one that matches your symptoms, X-rays, health risks, lifestyle, and goals. Bring a list of questions to your orthopedic appointment and ask what results you can realistically expect for your knee.



